]]>
• Bactericidal
• Inhibit bacterial DNA gyrase, topoisomerase IV, and two type II DNA topoisomerase enzymes
• For many gram-positive bacteria (such as S. aureus), topoisomerase IV is the primary activity inhibited by the quinolone (see gyrating dancers below)
• For many gram-negative bacteria (such as E. coli), DNA gyrase is the primary activity inhibited by the quinolone (see "queen" below stopping the gyrating dancers)
• Quinolones are well absorbed after oral administration and are distributed widely in body tissues
• Bioavailability: for the fluoroquinolones it is greater than 50% for all agents and greater than 95% for several
• Volume of distribution: (high) The concentrations of quinolones in urine, kidney, lung and prostate tissue, stool, bile, and macrophages and neutrophils are higher than serum levels. Quinolone concentrations in cerebrospinal fluid, bone, and prostatic fluid are lower than in serum.
• Excretion: Most quinolones are cleared predominantly by the kidney, and dosages must be adjusted for renal failure. However, pefloxacin and moxifloxacin are metabolized predominantly by the liver and should not be used in patients with hepatic failure.

ANTIMICROBIAL SPECTRUM
• bactericidal against: E. coli and various species of Salmonella, Shigella, Enterobacter, Campylobacter, and Neisseria
• Third generation fluoroquinolones : levofloxacin, moxifloxacin, and gatifloxacin. They possess antibacterial activity against Chlamydia, Legionella, and Mycoplasma species, streptococcal, staphylococcal pathogens, and variable activity against E. faecalis
THERAPEUTIC USES
• Prostatitis: Norfloxacin, ciprofloxacin, and ofloxacin
• Sexually Transmitted Diseases: activity in vitro against N. gonorrhoeae, C. trachomatis, and H. ducreyi
• Gastrointestinal infections: traveler's diarrhea (frequently caused by enterotoxigenic E. coli)
• Respiratory infections: Community acquired/atypical pneumonia ; gatifloxacin and moxifloxacin have activity against S. pneumoniae. Quinolones also have in vitro activity against the rest of the commonly recognized respiratory pathogens, including H. influenzae, Moraxella catarrhalis, S. aureus, M. pneumoniae, Chlamydia pneumoniae, and Legionella pneumophila
• Other infections: Ciprofloxacin received wide usage for the prophylaxis of anthrax and has been shown to be effective for the treatment of tularemia
• Urinary Tract Infection
ADVERSE REACTIONS
• Gastrointestinal: mild nausea, vomiting, and/or abdominal discomfort (3% to 17% of patients).
• CNS: mild headache and dizziness (0.9% to 11% of patients)
• Dermatology: Rashes; photosensitivity reactions
• Achilles tendon rupture or tendonitis (rare)
• Cardiac: QTc interval (QT interval corrected for heart rate) prolongation has been observed with sparfloxacin and to a lesser extent with gatifloxacin and moxifloxacin
• Endocrine: hypoglycemia has been reported in diabetic patients receiving insulin or glyburide plus fluoroquinolones
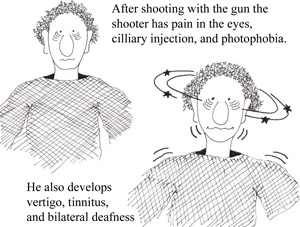
• combination of inflammatory eye disease and vestibuloauditory dysfunction
• rare autoimmune disorder affecting the inner ear
• described as Meniere's-like fluctuating hearing loss combined with impaired caloric response
• young adults commonly affected
• As many as 15% of CS patients have a large- to medium-vessel vasculitis
• As a helpful mnemonic device think of a man shooting a gun (rhymes with 'gan' in Cogan’s; see the side effects the shooter experiences in the figures below)
• acute nonsyphilitic interstitial keratitis
• sensorineural hearing loss (see figure 3 below)
• Medium- and large-vessel arteritis (aortitis, aortic regurgitation, coronary artery inflammation, mesenteric vasculitis, and limb claudication)
• severe vertigo (see figure 3 below)
• nausea/ vomiting
• tinnitus
• diarrhea and/or bloody stools (10% patients with CS)
DIAGNOSIS
• clinical suspicion (make sure to consider more common diseases before committing to a diagnosis of CS)
TREATMENT
• systemic corticosteroids for inner ear disease (high doses)
• topical steroids for interstitial keratitis
• cytotoxic agents for cases refractory to corticosteroids
DIAGNOSIS
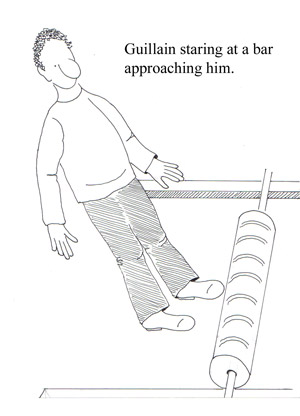
• a definitive diagnosis is usually not possible until the fifth day after the onset of symptoms
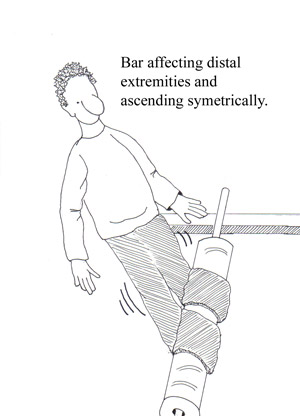
• Clinical features: progressive weakness in both arms and legs; areflexia
• CSF findings: elevated protein (greater than 0.55 g / dL ) without pleocytosis
• Electrodiagnostic findings: an absent H reflex, low amplitude or absent sensory nerve action potentials, an abnormal F wave, and other less frequent abnormalities
TREATMENT
• All patients who have GBS should be admitted to a hospital for close observation for respiratory compromise, cranial nerve dysfunction, and autonomic instability
• Monitor lung function
• Physical therapy
• Pain control with narcotics along with carbamazepine or gabapentin
• High-dose intravenous immunoglobulin (IVIg; 400 mg per kg daily for five days)
• Plasmapheresis (five exchanges over five to eight days) OR IVIG
• Porphyrias: a group of diseases caused by inborn enzymatic defects in the heme biosynthetic pathway
• Most common type of porphyria is PCT
• PCT results from a deficiency of hepatic uroporphyrinogen decarboxylase activity
• Acquired and Familial forms exist
o Acquired PCT: most often precipitated by alcohol, Estrogens, oral contraceptives, certain environmental pollutants, and iron overloading with accompanying genetic factors
o Familial PCT: autosomal dominant
• Aside: PCT has been suggested in some of the vampire and werewolf legends, hence the character below
• Blistering in sun exposed areas (caused by the generation of peroxide by the UV excited porphyrins)
• Increased skin fragility
• Facial hypertrichosis (see all figures)
• Hyperpigmentation
• Sclerodermoid changes
• Dystrophic calcification with ulceration
DIAGNOSIS
• “Port-wine urine”: red-brown discoloration due to high levels of porphyrin pigments
• Urine with a bright pink fluorescence under a Wood's light
• Elevated urine uroporphyrin: coproporhyrin ratio- a ratio of 4:1 or more
• Quantitative assays of the various porphyrins must be performed to obtain a reliable diagnosis
• Biopsy specimens for direct immunofluorescence are taken from the edge of lesions
TREATMENT
• Phlebotomy: iron removal because iron overload is one of the triggers of the disease. One unit of blood should be removed every 2 to 4 weeks until the hemoglobin drops to 10mirogm/dl or until the serum iron drops to 50micromg/dl.
Current guidelines for cholesterol treatment: http://www.nhlbi.nih.gov/guidelines/cholesterol/profmats.htm
Drug Treatment:
There are four major classes of medications are used to treat hyperlipidemia:
o HMG-CoA reductase inhibitors (statins)
o Bile acid sequestrants (cholestyramine, cholestipol)
o Nicotinic acid
o Fibric acids
o The statins can lower LDL levels by 18% to 55% and triglyceride levels by 7% to 30%. They also can raise HDL levels by 5% to 15%.Their major side effects include myopathy and an elevation of liver enzyme levels.
o The bile acid resins (cholestyramine, cholestipol) lower LDL levels by 15% to 30%, and raise HDL levels by 3% to 5%. They have no effect on triglyceride levels. Their major side effects include gastrointestinal distress, constipation, and a decrease in the absorption of other drugs.
o Nicotinic acid lowers LDL levels by 5% to 25% and triglyceride levels by 20% to 50%. Nicotinic acid also raises HDL levels by 15% to 35%. The major side effects of nicotinic acid include flushing, hyperglycemia, hyperuricemia, GI distress, and hepatotoxicity.
o Fibric acids lower LDL levels by 5% to 20% and triglyceride levels by 20% to 50%, and raise HDL levels by 10% to 20%. Their major side effects include dyspepsia, gallstones, myopathy, and unexplained noncardiac death.
o Hypertrophic cardiomyopathy (HCM) has classically been defined as hypertrophy of the myocardium greater than 1.5 cm without an identifiable cause.
o The disorder has a variable presentation and carries a high incidence of sudden death.
o The mortality rate for individuals with HCM is 4% per year.
o HCM is slightly more common in males than in females.
o HCM usually presents at an earlier age in females than in males.
Signs and Symptoms:
o patients with HCM may be asymptomatic.
o symptoms of HCM can include sudden cardiac death
o dyspnea
o syncope
o presyncope
o angina
o palpitations
o orthopnea
o dyspnea
o congestive heart failure
o dizziness
Death often is sudden and unexpected and typically is associated with sports or vigorous exertion. (see young athlete at the figure)
Physical Findings:
o The classic auscultatory finding for HCM is a crescendo-decrescendo systolic murmur along the left sternal border that increases with the Valsalva maneuver, (See the young athlete that is more powerfull while standing and with valsava maneuver, similarly squatting and hand grip decreases his power and the intensity of his murmur).
Imaging Studies:
o Two-dimensional echocardiography reveals LV hypertrophy and is diagnostic for HCM.
Procedures:
o Cardiac catheterization
o Electrophysiology studies
Surgical Care:
o Left ventricular myomectomy.
o Pacemaker implantation
o Catheter septal ablation
o Implantable cardioverter defibrillator
• Posttraumatic: occurs in approximately 3% of patients with spinal cord injury
SIGNS and SYMPTOMS
• Symptoms usually begin in the hands and arms (note swimmer diving in hands first)* because of the involvement of the central lower cervical spinal cord.
• Hyporeflexia in upper extremities: due to destruction of the dorsal horn fibers from muscle stretch receptors
• Loss of pain and temperature perception (hands and arms): destruction of dorsal horn fibers from pain receptors
• Position, vibration, and touch sensation are usually preserved
• Upper extremity muscle weakness and atrophy: destruction of motor neurons and the anterior gray horns
• Lower extremity spastic weakness: occurs as long ascending and descending pathways are compressed by the expanding syrinx
• As the syrinx increases in diameter, long ascending and descending pathways passing through the involved cord segment are compressed or invaded by the cavity and cause spastic weakness of the legs. Tracts to and from the sacral bladder centers are spared, or involved late in the disease, so that bladder symptoms occur late or not at all.
• Central neuropathic pain
• Headache and neck pain
• Autonomic symptoms (interruption of intermediaolateral column): Horner’s syndrome and trophic changes of the skin
DIAGNOSIS
• Spinal MRI with contrast : reveals a central spinal cord cavity
• Electrophysiology: denervation in affected segments
TREATMENT
• Neurosurgical: Budd Chiari malformation – foramen magnum decompression
Posttraumatic - shunt
• Types
o MEN I: tumors involving the parathyroid glands; endocrine pacreas; and the pituitary
o MEN IIA: medullary carcinoma of the thyroid gland; pheochromocytoma; and hyperparathyroidism
o MEN 2B: medullary carinoma of the thyroid; multiple neuromas; and pheochromocytoma
• Autosomal dominant
• 2-20/100,000
• features:
o hyperparathyroidism*
o enteropancreatic tumors (gastrinomas/Zollinger-Ellison syndrome; VIPomas; glucagonomas; insuilinomas)**
o pituitary adenomas (prolactinomas)***
o adrenal adenomas
o carcinoid tumors
o facial angiofibromas
*Note: Predator attacking victim’s parathyroid (hyperparathyroidism)gland by grasping either side of the victim’s neck
**Note: Predator attacking the victim by kicking him to the abdomen inducing tumors.
***Note: Predator attacking the victim’s pituitary gland by poking the victim between his eyes inducing pituitary adenoma.
• Symptoms are related to the respective tumors
• Treatment
o Hyperparathyroidism
• Partial or total resection of parathyroid glands
• Prophylactic thymectomy
o Gastrinomas
• Proton pump inhibitors
• Correction of hypercalcemia
MEN II
• Autosominal dominant
• 1-10/100,00
MEN IIA (Sipple’s syndrome)-like sheep
• features
o medullary carcinoma of the thyroid (80-100%)*
• calcitonin producing parafollicular cells
o hyperparathyroidism**
o pheochromocytoma (50%)
• Hypertension; headache; palpitations; diaphoresis
• Super-strength demonstrated by the sheep after conquering the victim indicates the elevated catacholamines ***
o Hirschsprung’s disease
*Note: Sheep attacking victim’s thyroid resulting in medullary thyroid carcinoma
**Note: Sheep attacks parathyroid gland resulting in hyperparathyroidism
***Note: Sheep has power after eating the very nutritional thyroid and parathyroid organs and develops pheochromocytoma
MEN IIB (MEN III)
• Features
o Medullary carcinoma of the thyroid*
o Pheochromocytoma**
o Marfanoid body habitus
o Multiple neuromas of the conjunctiva; lips; labia; tongue; mucosa; larynx***
*Note: Werewolf attacking victim’s thyroid resulting in medullary thyroid carcinoma.
**Note: Werewolf now becomes very powerfull immediatelly, and develops pheochromocytoma after eating the thyroid gland.
***Note: Werewolf develops neuromas from all the energy produced from the pheochromocytoma.
• Still's disease is a form of arthritis that is characterized by high spiking fevers and transient
salmon-colored rash.
• First described in children, but it is now known to occur, much less commonly, in adults
• Possible Pathogenesis: Infection; hypersensitivity; or autoimmune disorder
• Extreme fatigue
• Waves of high fever 104 degrees F (41 degrees C)
• Faint salmon color skin rash comes and goes usually doesn’t itch.
• Inflammation of the lungs (pleuritis)
• Inflammation of the pericardium (pericarditis)
• Fluid accumulation around the lung (pleural effusion)
• Inflammation of the liver
• Sore throat
• Arthritis this usually involves many joints (polyarticular arthritis).
DIAGNOSIS
• Persistent arthritis (arthritis lasting at least 6 weeks)
• Markedly elevated white blood cell count
• Low red blood count (anemia)
• Elevated ESR
• Rheumatoid arthritis (rheumatoid factor) and systemic lupus erythematosus (antinuclear antibodies, ANA) are usually negative. Other diseases especially infections, cancer, and other types of arthritis are excluded
TREATMENT
• Aspirin or other non-steroid drugs (NSAIDs)
• Steroids such as prednisone, are used to treat more severe features of illness.
• Persistent illness: medications that affect the inflammatory aspects of the immune system are used.
These include:
• Hydroxychloroquine (Plaquenil)
• Penicillamine
• Azathioprine (Imuran)
• Methotrexate (Rheumatrex)
• Cyclophosphamide
• Etanercept (Enbrel)
• Infliximad (Remicade)
• Corticosteroids
• Osteoarthritis (OA ) is degenerative disease more common in older adults
• Approximately one millon people affected
• Morning stiffness less than 30 minutes
• Pain exacerbated with movement
• Rare systemic involvement
• Minimal joint inflammation
• Bony enlargement of the affected joint
• Pain and/or deformity in the distal and proximal interphalangeal joints (DIP and PIP)
(see figures 1A and 1B)
• Radiographic findings: narrowing joint space; osteophyte formation; sharpened articular margins; dense subchondral bone (absence of radiographic findings does not exclude the diagnosis)
SIGNS
• Nodes: bony enlargements of the affected joints
• BOUCHARD nodes occur at the PIP joint (think of a BUTCHER grasping the knife using his PIP joint
as he chops meat; see Fig. 1A)
• HEBERDEN nodes occur at the DIP joint (think of a gardener picking HERBS using his DIP joints)
• Limited range of motion
• Crepitus on motion
Heberden nodes occur at the DIP joint (Think of a gardener flexing his DIP joints while picking herbs)
TREATMENT
• Nonpharmacological: weight reduction; exercise; and joint protection.
• Initial pharmacological treatment: acetaminophen and capsaicin, (.025%)
• Moderate pain: Non steroidal anti-inflammatory agents (NSAIDS).
• Severe pain: steroid injections( ie. 40mg Triamcinolone) into the most severely affected joint;
Hyaluronic acid-like product joint injections
• Surgical intervention: joint replacements for moderate to severe pain and functional impairment
.
• 1793: Tilesius von Tilenau first described neurofibromatosis.
• 1849: R. W. Smith further described it.
• 1882: von Recklinghausen was the first person to associate the origin of this disorder to tumors
arising from cells of the nerve sheaths.
• 1880s: Joseph Carey Merrick in London known as the “elephant man” because of his disfiguring
deformity of the head, extremities, and vertebral column.

DIAGNOSIS (2 or more of the following criteria)
• More than 6 café-au-lait spots measuring at least 15 mm in adults and 5 mm in children
(Café-au-lait spots are found in more than 50% of individuals with NF1.)
• At least 2 or more neurofibroma of any type or at least 1 plexiform neurofibroma
• Freckling in the axillary or inguinal regions
• Optic glioma
• Two or more Lisch nodules (iris hamartomas) (VonRecklingenhausen is eating Lindt chocolates)
• A distinctive bony lesion, such as sphenoid wing dysplasia or thinning of a long bone with or
without pseudoarthrosis
• A first-degree relative with NF1, as suggested by these criteria
SIGNS
• spinal deformities: scoliosis and kyphoscoliosis.
• congenital bowing and pseudoarthrosis of the tibia and the forearm.
• overgrowth phenomenon of the extremity.
• soft tissue tumors
TREATMENT
• Plastic surgery to correct disfigurement
• Surgical treatment of intraspinal or intracranial tumors, and tumors of the peripheral nerve